
ANTI MICROBIAL APPLICATIONS OF ANOLYTE IN DENTISTRY
Scientists exploring infection control problems have been discovering an alarming amount of evidence regarding the safety of the water that is sprayed into the mouth from dental instruments.
A recent study documented in the Journal of the American Dental Association concluded that
“Microbial contamination of dental unit water appears widespread and extensive, and the organisms populating the water lines include many with pathogenic potential which can cause serious illness and death, especially when the immune systems are down”
Among the recent findings: standard microbial culture techniques, as well as new analytical techniques, have revealed extraordinary numbers of a wide variety of waterborne “opportunistic” pathogens. These bacteria are quick to take advantage when the immune system defenses are low, with immuno-compromised patients especially at risk. The bacteria found in dental water lines may cause significant infection in these individuals.
Legionella, the bacteria which cause Legionnaires’ disease, are present in dangerously high concentrations in the majority of dental chairs.
The source of these maverick bacteria which inhabit the dental unit water lines is two fold. First, research indicates that the majority of the organisms originate in the municipal water system. Conventional municipal water treatment procedures are proving inadequate in dealing with a wide variety of these “super bugs”.
The tiny dental water lines provide a large interior surface area combined with low flow rates and stagnation, two ideal conditions for the formation of a thin slime of microbes called “biofilm” on the interior surfaces of the dental lines.
BIOFILM GROWING IN DENTAL WATERLINE
This dental water biofilm is an accumulation of dozens of types of microorganisms stacked and interwoven with each other in a cooperative ecosystem. Layer upon layer of these microbes grow on the inner surface of the dental water line until occasionally a “clump” breaks free and enters the patient’s mouth.
The second source is known as the “suck back” effect, caused by imperfect anti-retraction valves in dental instruments, thus permitting the withdrawal or “suck back” of blood, saliva and other materials from a patient’s mouth into the waterline. Research studies have identified a wide range of bacteria resident in the biofilm which originated in patient’s mouths.
The methodical sterilization of dental instruments between patients providing sterile instruments thus fails to prevent potential pathogens from flowing from the dental water lines through the newly cleaned instrument into the next patient’s mouth. Research studies have clearly shown that efforts to “flush” the water lines between patients are ineffective in removing the biofilm. In fact, flushing leads to incredibly fast re-growth rates due to new organisms and “food” being supplied to the biofilm during the flushing procedure.
Chemical rinses have also proven to be less than effective. Increasing chemical dosages to lethal levels for the biofilm endangers the patient as well as the dental care givers themselves, especially when residues of these chemicals may directly enter the bloodstream during certain invasive procedures.
Concern about the biofilm problem and the potential dangers of bacterial infections originating from municipal water systems has led some governments to mandate the use of sterile water for all dental surgical procedures. Considering total CFU measurements in randomly selected dental offices generally reach into the hundreds of thousands, and sometimes 1-3 million CFU/ml, this poses a potentially serious and formidable problem for all professionals involved in general dentistry.
In this situation, the dentist (oral surgeon) either purchases bulk distilled water or uses a small steam distiller to produce a couple of gallons of steam distilled water each day. The sterile distilled water is placed in a pressure vessel and then fed into the dental water lines during normal dental procedures. This process is designed to isolate the dental patient, water lines and dental instruments from the municipal water supply, and additional bacterial contamination from that direction.
Unfortunately, the use of sterile water by itself does not ensure a bacteria free dental water line. Studies have shown that even pressurized distilled water sources can be contaminated by suck back effects and other environmental(handling) activities.
The use of anolyte will solve the safety water general dentistry problem by incorporating a combined water purification(distillation) system with a water altering/structuring system which will provide a biocidal capability for all water used in the dental office waterlines leading to the patient. The target of bacteria free water can be met with a “free-standing” water treatment unit and without the use of any point-of-use(POU)filtration devices which are designed to remove all bacteria.
Contamination which may come by way of “suck back” effects will also be contained by the disinfected water which is entering the system. By maintaining a continual residual of biocidal in the dental waterlines, it will be easy to maintain the 0 CFU/ml total bacteria count.
The dentist now can attain the bacteria free water target without ripping out his or her entire water system or paying for replacement filters on a daily or weekly basis; the oral surgeon can now have organic, inorganic and microbe-free water in his water delivery system without worrying about suck-back or internal/handling contamination problems which would corrupt that water purity.
In most cases, special approvals are required only if a piece of dental equipment is “hard wired” into the system. In the present case, the disinfecting agent -anolyte- could be produced by a stand-alone unit which would be capable of servicing several operatories. Being physically independent of the existing dental equipments will make it easier for integration into dental operations. Whether or not any government approval is needed is subject to discussions with local authorities.
OVERVIEW OF SYSTEM AND OPERATIONAL INTERFACES
Although the anolyte disinfected water water technology has potential many applications in the dental area(mouthwash, surface cleaner, instrument cleaner, toothpaste, periodontal and oral surgery sterilant, and others), initial development efforts using electrolyzed water should initially focus on the application of this technology to the dental waterline biofilm problem.
TYPICAL INSTALLATION OF ANOLYTE GENERATOR SYSTEM FOR DISINFECTIOON OF DENTAL UNITS WATER LINES





|
Dental Clinic |
ELA-200ANW unit |
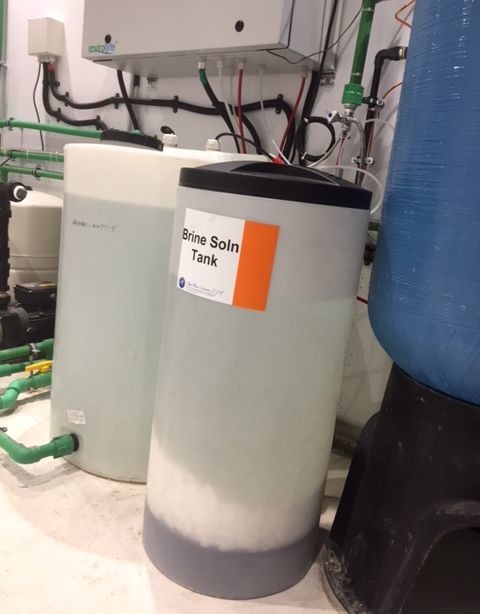
Anolyte storage tank with dosing pump |
Brine tank |
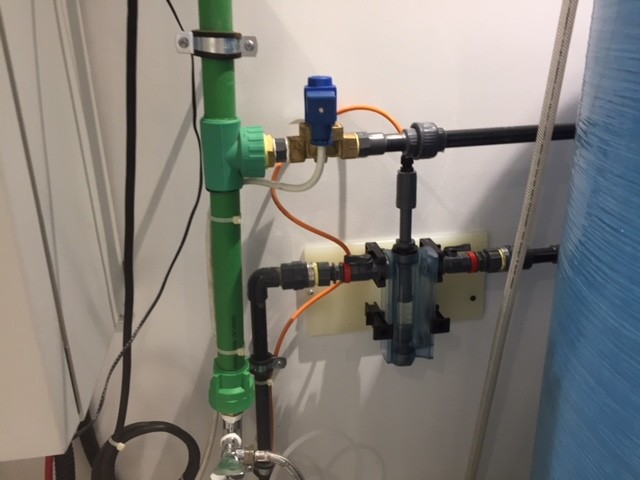
Anolyte dosing pump |
Flow sensor |
Water lines to dental units |
ALTERNATIVES TO ANOLYTE
With the increased attention being focused on dental water line contamination, a wide variety of “solutions” have hit the market some with government approval, some without approval.
With the exception of removable water bottles which are used to feed sterile, distilled water into the waterlines, there are no other stand-alone systems which are on the market
For brevity’s sake, all water bottle systems are susceptible to microbial growths and do not ensure that existing biofilm in attached control system and waterlines will not migrate into patient’s mouth.
Disinfection of dental units water lines with anolyte in a dental clinic in Abu–Dhabi
Susceptibility of E. faecalis to different electrochemically-activated solutions in comparison with contemporary irrigants with and without the addition of EndoActivator
M. B. Akbulut
DDS, Research Assistant, Department of Endodontics, Faculty of Dentistry, Selcuk University, Konya, TURKEY
A. U. Eldeniz
DDS, Ph.D, Associate Professor, Department of Endodontics, Faculty of Dentistry, Selcuk University, Konya, TURKEY
Aim: To assess and compare antimicrobial efficacy of different electrochemically-activated solutions (ECA) and contemporary irrigants in root canals infected with Enterococcus faecalis when used with or without the EndoActivator (EA).
Methodology: Crowns and apical portions of 100 extracted single-rooted human teeth were removed. The root canals were instrumented with ProTaper files to size F3 and sterilized. Ninety root segments were infected with E. faecalis for four weeks and divided to eight test groups (n=10) (four without EndoActivator sonication and four with) and the positive control (n=10). Tested irrigants were electrochemically-activated solutions produced by Medilox® device (ECA-MX) and Envirolyte® device (ECA-EN), 2% CHX (Drogsan, Turkey) and 2.5% NaOCl (Caglayan Kimya, Turkey). Root specimens were irrigated with 5 mL of the test solution and in EA groups additionally sonic agitation was applied. Ten samples were used to check the sterility (negative control). Dentine samples that were obtained from the walls with gates-glidden burs (# 3, 4, and 5) were cultured and the antibacterial efficacy was evaluated by counting colony-forming units. Data were statistically analysed with Kruskal-Wallis and Mann Whitney-U tests (α = 0.05).
Results: ECA-EN, 2.5% NaOCl and 2% CHX were all clearly more effective agents in killing E. faecalis than ECA-MX (P < 0.05). Addition of EndoActivator sonication to experimental irrigants demonstrated no statistical difference in the elimination of E. faecalis (P > 0.05).
Conclusion: Within the limitations of this ex vivo study it can be concluded that ECA-EN may have potential as an endodontic irrigant with favorable results while EndoActivator usage gives no benefit in reducing bacteria from the root canals.